A hospital-employed physician at 58 with $2 million in a 401(k) and a $150,000-per-year pension faces a retirement tax problem most planning guides miss. The pension creates a permanent income floor that compresses the window for Roth conversions, limits control over taxable income in early retirement, and nearly guarantees IRMAA surcharges once RMDs begin. The three moves that matter most: rebalance toward inflation-resilient equity, convert aggressively before the pension income floor locks in, and model the gap years with precision.
The Pension Compression Problem that Most Physicians Don’t Model
Generic Roth conversion advice tells physicians to convert up to the top of the 22% bracket for married filing jointly, which runs to $211,400 in 2026. That bracket ceiling assumes the only income is the conversion itself. A physician with a $150,000 pension has already consumed most of that space before converting a single dollar.
The 22% bracket for married filing jointly tops out at $211,400. Subtract $150,000 in pension income, and the remaining conversion room is $61,400 before crossing into the 24% bracket. A physician without a pension can convert more than three times that amount at the same marginal rate. Over a decade of gap years, that difference compounds into hundreds of thousands of dollars in a pre-tax account, waiting to be taken as RMDs.
A $2 million traditional 401(k) will produce a meaningful RMD at age 73 under current IRS Uniform Lifetime Table factors. Stack that on a $150,000 pension, and the combined income reaches $230,000, well into the 24% bracket ($211,400 to $403,550 for MFJ in 2026). That income level also crosses the second IRMAA tier, triggering $2,886 per person annually in combined Part B and Part D surcharges on top of the standard $202.90 monthly Part B premium. For a married couple, the annual IRMAA hit reaches $5,772.
The Gap Years: The Window That Closes Faster Than Expected
The gap years span from retirement to Medicare eligibility at 65 and to RMD age at 73. For a physician retiring at 60, that window is roughly 13 years, but for one retiring at 62, it is 11 years. This is the only period where income is genuinely controllable.
A physician with a $150,000 pension, retiring at 60, still has $61,400 in annual conversion room in the 22% bracket. Converting that amount each year for 10 years moves $614,000 out of pre-tax status, meaningfully reducing the eventual RMD base and IRMAA exposure. Converting above the 22% ceiling is worth modeling: paying 24% now to avoid 24% plus IRMAA surcharges plus potential Social Security taxation later can produce a lower lifetime tax burden, depending on the timeline.
The IRMAA two-year lookback makes this urgent. IRMAA uses income from two years prior, so a large conversion in 2026 affects 2028 Medicare premiums. Physicians who delay conversions until the year before Medicare enrollment have already lost two years of planning runway.
Allocation: Enough Equity to Outrun Inflation Over 25 Years
A physician retiring at 60 faces a potential 25 to 30-year retirement horizon. The Consumer Price Index has risen from 319.785 in March 2025 to 327.46 in February 2026, and core PCE, the Fed’s preferred inflation measure, has risen steadily from 125.267 to 128.394 over the same period. A portfolio shifted too heavily into fixed income at retirement will lose purchasing power over that horizon.
The 10-year Treasury yield sits at 4.44%, offering meaningful income from fixed-income allocations. But a physician with a $150,000 pension already holds a large fixed-income-equivalent position. That pension functions like a bond paying $150,000 annually. A heavily bond-weighted 401(k) on top increases exposure to interest rate and inflation risk.
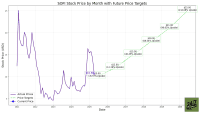
Dividend-oriented equity allocations provide income without eliminating growth. Schwab U.S. Dividend Equity ETF (NYSEARCA:SCHD | SCHD Price Prediction) currently yields around 3.46%, generating approximately $80,000 annually on a $2 million position. JPMorgan Equity Premium Income ETF (NYSEARCA:JEPI) yields around 8.43%, though its covered-call structure limits upside participation. A balanced allocation between growth-oriented dividend funds and fixed income allows the portfolio to keep pace with inflation while the pension handles baseline income.
Three Planning Variables Worth Modeling Before Retirement
- Roth conversion room is calculated by subtracting pension income from the top of the current bracket. For a married physician with a $150,000 pension, the 22% ceiling in 2026 leaves $61,400 of room. Bracket thresholds adjust for inflation each year. If the combined income will cross the first IRMAA threshold of $109,000 for single filers or $218,000 for joint filers in retirement, converting above the 22% ceiling may still be worth the current tax cost.
- The gap years between retirement and age 73 represent the period where income is most controllable, and each year can be assigned a conversion target. The two-year IRMAA lookback means conversions done today affect Medicare costs two years after enrollment. A physician retiring at 60 who converts heavily at 62 and 63 will see elevated IRMAA costs at 65 and 66, a trade-off worth pricing explicitly before committing to a conversion schedule.
- Equity exposure sufficient to outpace inflation over a 25-year horizon is a factor in long-term portfolio construction. A $150,000 pension covers baseline expenses for many physicians, so the 401(k) can tolerate more equity volatility than a portfolio that supports all living expenses. The Fed Funds rate at 3.75% and a 10-year Treasury at 4.44% offer reasonable fixed-income yields today, but locking in duration risk at the start of a 25-year retirement exposes the portfolio to purchasing power erosion if inflation persists.