Alex Karnal, co-founder and CIO of Braidwell, a life sciences investment firm, spent 20 years building and backing biotech companies before declaring on the Invest Like the Best podcast that “2025 was probably the single most exciting year in my entire journey.” The catalyst: GLP-1 medicines. His claim deserves scrutiny because the investment and personal health implications are substantial.
A Trillion-Dollar Claim Worth Examining
Karnal’s argument has two parts. First, the commercial case: “This is a class of medicines that will easily be in excess of $100 billion a year in revenue.” Second, the structural case: GLP-1 adoption is “the first commercial proof that we are ready for what I think we’re gonna look back on in time as a once-in-a-lifetime trillion-dollar revolution in all of public health.” He frames this not as a pharmaceutical success story but as a behavioral shift, with consumers “voting with their feet” to move from reactive disease treatment to proactive health protection.
The structural case is harder to price: GLP-1 adoption as a behavioral shift toward proactive health is a compelling framework, but the timeline and policy environment remain genuinely uncertain.
The Commercial Case Has Real Numbers Behind It
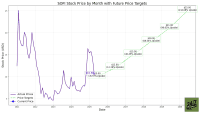
Eli Lilly (NYSE: LLY | LLY Price Prediction) generated combined GLP-1 drug sales of $36.5 billion in 2025, comprising around 56% of the company’s total revenues. Its stock has gained 11% over the past year and an extraordinary 407% over five years. Peer-reviewed research published in 2025 confirmed that GLP-1 medicines “improve outcomes in people with cardiovascular, kidney, liver, arthritis, and sleep apnea disorders” through anti-inflammatory and metabolic pathways, with some benefits occurring independently of weight loss itself.
GLP-1 drugs were designed for blood sugar control in Type 2 diabetics, but their benefits in cardiovascular disease, kidney disease, and metabolic liver disease emerged from trials rather than intent, which is part of what makes the platform so unusual.
Forecast Cuts and Competitive Pressure Complicate the Picture
Karnal’s $100 billion annual revenue floor is credible, but the path there is messier than the podcast framing suggests. Analysts at Jefferies revised down their forecast for the weight-loss market to a peak of $80 billion from an earlier estimate of over $100 billion by the early 2030s. Goldman Sachs pegged global obesity drug sales at $105 billion by 2030, down from earlier forecasts of $130 billion, citing steeper price erosion. The $150 billion figure that Wall Street once treated as a floor has shifted to a 2035 target for some analysts.
The headwinds are specific. Novo Nordisk (NYSE: NVO) stock is down nearly 20% year-to-date and 29% over the past year, hit by a clinical trial setback where its CagriSema drug showed 23% weight loss versus Lilly’s tirzepatide at 25.5%. Medicare coverage for GLP-1 obesity drugs remains unresolved, with major insurers, including CVS, opting out through at least this spring. Semaglutide’s patent expired in India in March 2026, enabling generic competition at steep discounts.
The market’s trajectory depends heavily on policy decisions, patent timelines, and which companies execute best.
Time Horizon Determines Whether This Thesis Works for You
Karnal’s framework is most useful for investors with a long time horizon, specifically those comfortable holding positions for a decade or more. The oral pill format is accelerating adoption: Lilly’s newly approved Foundayo drew 1,390 prescriptions in its first week on the market, removing injection barriers and expanding the addressable population. For a long-term investor, the structural argument that GLP-1s represent a platform for proactive health management rather than a single-indication drug is worth taking seriously.
For investors with shorter time horizons or concentrated positions in a single GLP-1 name, the risks are asymmetric. Novo Nordisk shareholders who held through the CagriSema failure in February 2026 experienced a 15% single-day drop. The competitive dynamics between Lilly and Novo, plus the entry of new competitors, including a major e-commerce platform’s GLP-1 management program and a large pharma company’s monthly-injection candidate in Phase 2b, mean that picking the right company matters as much as picking the right sector.
The Health Stack Framework
Host Patrick O’Shaughnessy introduced the concept of a “Health Stack” during the conversation, borrowing from technology, where “your tech stack is all the various components that you use to create your overall thing.” The framing positions GLP-1 adoption as one layer in a broader individual health optimization strategy, alongside glucose monitoring, cardiovascular screening, and preventive interventions.
For investors, the practical implication is that the GLP-1 opportunity extends well beyond drug manufacturers. Diagnostic companies, delivery platforms, and insurers who figure out coverage structures will all be shaped by the same trend Karnal is describing. His point that “the gap is not necessarily needing more medicines, it’s actually pointing those medicines at the impact that they can have” is an argument for the entire ecosystem around drug delivery and patient adoption, not just the molecules themselves.
What remains contested is the timeline, the winners, and whether the policy environment will accelerate or delay adoption — the scientific foundation is solid, but that alone does not determine who profits or when. Investors who treat GLP-1s as a confirmed trillion-dollar outcome rather than a trillion-dollar opportunity with meaningful execution risk are the ones most likely to be surprised by the volatility already underway.